"Living an ocean away, I used to worry every single day.
Now I see Dad's wellbeing in real time."
Lilo speaks with my father in his first language every morning. The family portal shows mood patterns, engagement, and alerts for early signs of withdrawal — so the care team can intervene before small concerns become crises.
— Illustrative scenario based on early pilot conversations. Composite, not an individual user.Lilo Solace
A deterministic safety pipeline designed to surface and de-escalate mental-health crises in assisted-living residents — engineered for the moments that can't be missed.
A Crisis That Can't Be Solved With Human Labor Alone
The convergence of mental health prevalence and workforce collapse demands a new paradigm
The Staffing Paradox
When staff are unavailable, care retracts to basic physiological needs—feeding, toileting, medication. Psychosocial needs become "luxuries" that can't be afforded. This strips residents of meaningful connection, reinforcing isolation and accelerating decline.
The industry is mathematically incapable of solving this crisis with human labor alone. A paradigm shift is required.
Prevents Crises. Saves Lives. Scales Care.
Deterministic safety pipeline with 5 evidence-based therapeutic skills
Crisis Prevention
100% recall rate—zero false negatives in detecting mental health crises before escalation
Family Connection
Transparent wellness dashboards keep families engaged with real-time updates on mood, activities, and health patterns
Staff Efficiency
Automated assessments and proactive alerts free caregivers to focus on meaningful human connection
Financial Impact
Proven cost savings through reduced hospitalizations, lower readmission rates, and improved quality metrics
Three Steps. Profound Impact.
From conversation to crisis prevention in under 3 minutes
Senior Speaks Naturally
Voice-first interface with 3-second pause tolerance, hearing aid compatibility, and medical vocabulary
Technical Details
- Whisper STT + Piper TTS = $0 API costs
- 95%+ accuracy for senior voices
- Background noise filtering
AI Analyzes & Responds
Five-layer deterministic pipeline. 100% recall on the internal safety-test suite, sub-second crisis detection latency on cloud and edge hardware.
See Pipeline Layers
- L1: Guardian — PII redaction + 4-gate deterministic crisis detection
- L2: Cognitive Kernel — intent classification across 11 categories
- L3: Clinical Services — 13-instrument clinical assessment framework
- L4: Empathy Engine — 7 evidence-based therapeutic skills + LLM generation
- L5: Reflector — safety validation + hallucination detection
Care Team Alerted
Real-time notifications with severity-based routing and SLA timer tracking
Platform Details
- 16-service architecture (13 Docker containers + 3 host processes)
- HIPAA §164.312 technical safeguards implemented; 7-year audit-log retention
- HL7 FHIR R4 integration: code-ready, not yet enabled in production
- Severity-based routing and SLA timers in the alert pipeline
Technology Deep Dive
Enterprise-Grade Architecture
Built from scratch with healthcare-grade reliability and scalability
Deployment Architecture ↓
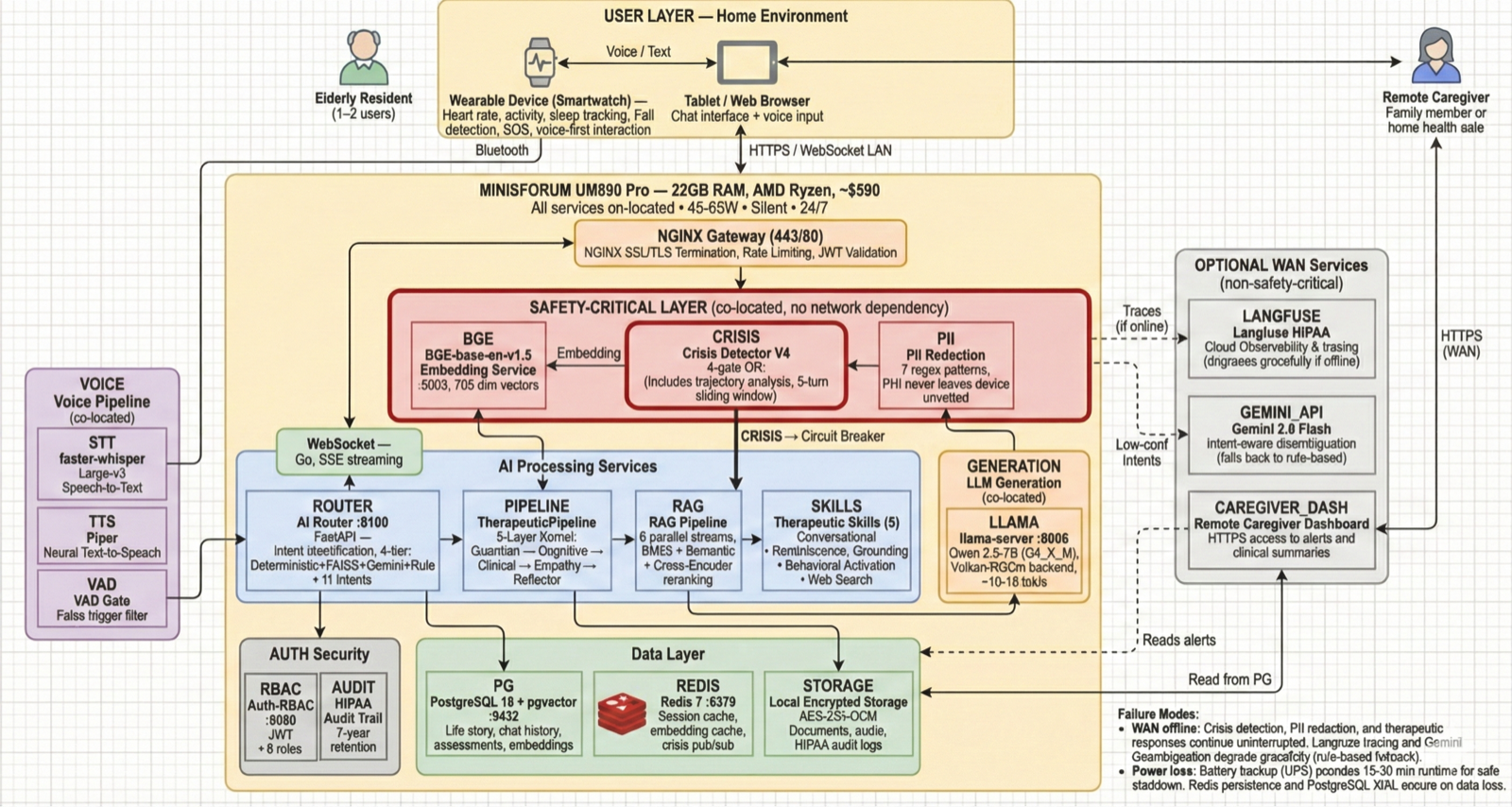
At-Home Care (1–2 users) — Minisforum UM890 Pro 32GB, ~$590. Full stack on one silent box. All safety-critical models co-located. 45-65W, shelf-mountable.
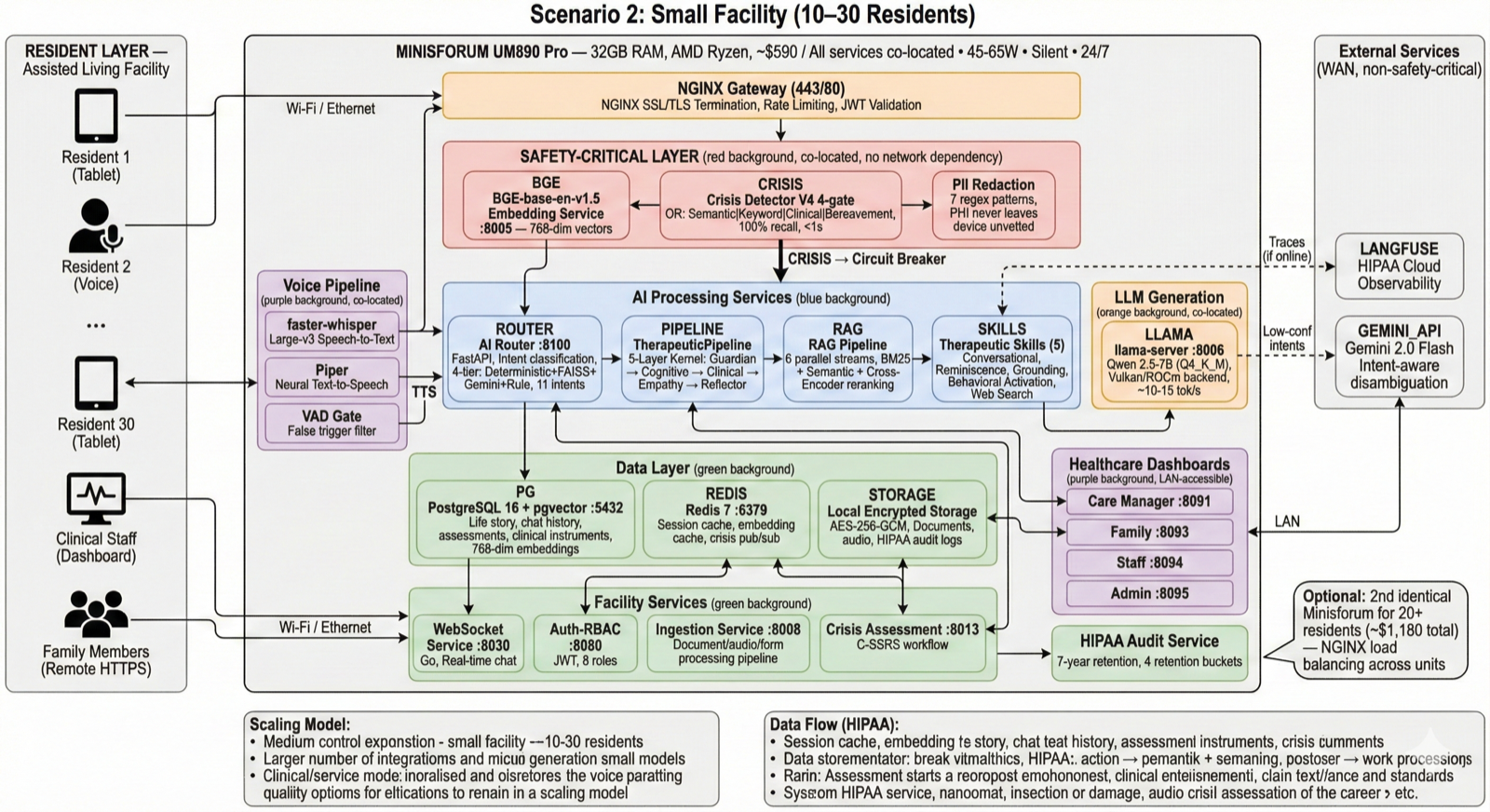
Small Facility (10–30 residents) — 1-2× Minisforum edge devices ($590–$1,180) with NGINX load balancing. Each runs full safety stack independently. Central server for dashboards and persistent storage.
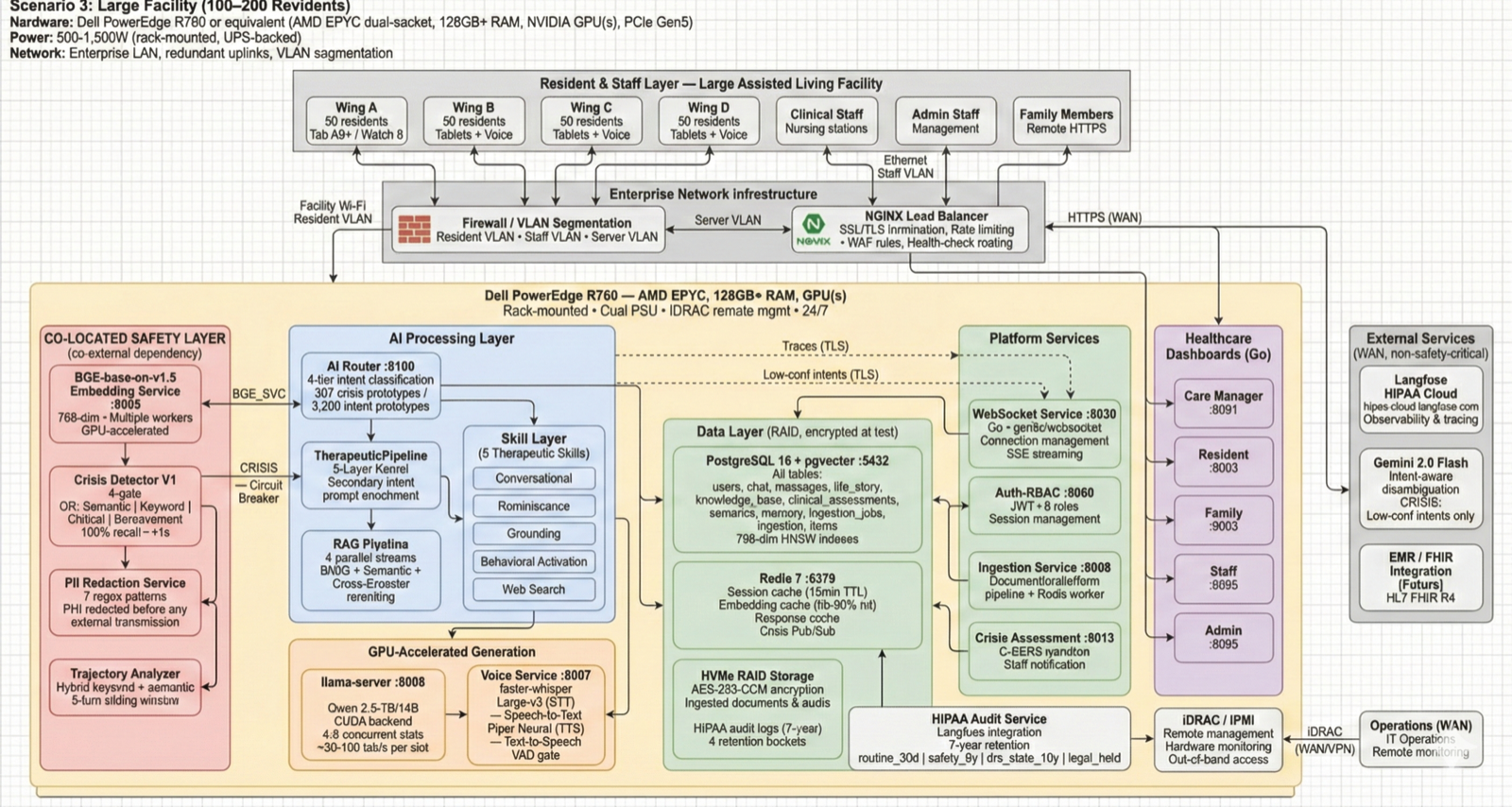
Large Facility (100–200 residents) — Dell PowerEdge R760, AMD EPYC, 128GB+ RAM, NVIDIA GPU(s), $3,000–$8,000. Multi-GPU inference, VLAN segmentation, dual PSU, iDRAC remote management.
Guardian → Cognitive → Clinical → Empathy → Reflector
13 Docker containers + 3 host processes
All on-premise, zero cloud dependency for safety
Why Pipelines, Not Agents
Safety by Architecture, Not Convention
Agentic AI systems exhibit 0.5–2% failure rates. In a facility handling 100 interactions/day, that means potentially missing one crisis every two days. We eliminated this risk entirely.
Agentic Orchestration
- Crisis detectionConvention (bypassable)
- Execution paths7+ variable
- LLM calls/request1–3+ (variable)
- Audit trailNon-deterministic
- Failure modeSilent reasoning errors
- Response time7–20+ seconds
Deterministic Pipeline (Lilo)
- Crisis detectionStructural invariant
- Execution pathsExactly 2
- LLM calls per requestExactly 1 (Layer 4)
- Audit trailDeterministic (L1→L5)
- Failure modeExplicit stage failures
- Response time2.64 s mean on L4 cloud
Our core design principle: safety must be enforced through structural invariants that cannot be bypassed regardless of system state — not through conventions that degrade as code complexity grows.Learn more about our research →
13 Clinical Instruments, Integrated
Scoring implementations aligned to the published protocols
A three-tier framework that feeds directly into the crisis detection gates. "Validated" here means the scoring logic conforms to the published protocols (PHQ-9, GAD-7, C-SSRS, and the rest) — clinical outcome validation is the job of the pilot.
Every resident, scheduled intervals
On clinical indication, feeds crisis detection
Baseline + 90/180 days, track trajectories
Cloud SaaS or on-premise edge
Crisis detection never depends on the internet.
Cloud SaaS is the default — fastest to get going. On-premise is available for facilities that need data sovereignty or offline safety guarantees. On the edge option, all services and models run locally on a single device; patient data never leaves the premises.
Architectural Invariant: Model Co-Location
All safety-critical models (BGE embedding + SLM generation) are co-located on every device. Crisis detection never depends on network connectivity. If the internet goes down, the device continues all operations autonomously — crisis detection, therapeutic response, storage, and dashboards all remain fully functional.
Minisforum UM890 Pro barebones ($479) + 32GB DDR5 ($60) + 1TB NVMe ($50)
Crisis detection, embeddings, and LLM generation all run locally on-device
HIPAA §164.312 compliant with TLS 1.3 + AES-256 encryption
Silent, fanless 24/7 operation — fits on a shelf or wall-mount
Scales From Home to Enterprise
Full stack on one silent box. 45-65W, shelf-mountable. Models ~7-8GB + services ~4-6GB + OS ~3-4GB = 14-18GB used, 14-18GB free.
Peak 3-5 concurrent users. Each unit runs the full stack independently with NGINX load balancing. 2 LLM slots per device.
15-30 concurrent users. Multi-GPU inference, 128GB+ RAM, dual PSU, remote management via iDRAC. Enterprise reliability.
Cross-platform by design: Model weights (GGUF format) are portable across Metal, CUDA, Vulkan, and ROCm backends. Same deterministic pipeline, same safety guarantees, any hardware.
Our path to clinical evidence
Engineered today. Clinically measured next.
We are not in a position to claim clinical outcomes yet — the pilot is designed to produce them. Here is exactly where we are, and how we get there honestly.
What has been validated
The engineering. The deterministic safety pipeline, the 4-gate OR crisis detection, sub-second detection latency on cloud and edge hardware, 100% recall on our internal 456-test safety suite, scoring implementations for 13 clinical instruments aligned to their published protocols, HIPAA §164.312 technical safeguards with 7-year audit-log retention, and row-level-security multi-tenancy tested on 61 entity tests.
No Lilo-generated clinical outcomes exist yet. Any effectiveness associated with the therapeutic methods we use comes from the published literature on those methods — behavioral activation in geriatric depression (Cuijpers, Dimidjian), reminiscence therapy (Pinquart & Forstmeier), grounding (Najavits, van der Kolk), and the C-SSRS suicide-risk assessment. Lilo's pilot measures whether delivering those methods through an AI companion produces the effects reported in the source literature.
Feasibility pilot
- Design — single-arm feasibility study (not an RCT)
- Sample — n = 20 residents at 1–4 facilities, 90-day intervention
- Primary endpoint — PHQ-9 change at 90 days
- Secondary endpoints — GAD-7, UCLA-3, WHO-5 change; engagement; safety events
- IRB submission — targeted June 2026
- Enrollment — Q3 2026, pending IRB approval
- Preliminary results — Q4 2026 / early 2027
Prospective evidence study
- Sample — n = 100, prospective, Aug 2026 – Mar 2027
- Purpose — primary efficacy data for the FDA evidence package
- Endpoints — PHQ-9, GAD-7, UCLA-3, WHO-5; safety; engagement
- Design — controlled (historical or concurrent, per IRB protocol)
Randomized controlled trial
- Sample — n = 200 randomized, multi-site
- Timing — starts after FDA clearance (Jul 2027 design, Aug 2027 launch)
- Purpose — definitive evidence for guideline inclusion
Regulatory path
FDA De Novo pathway. Pre-submission meeting targeted Q3 2026; De Novo submission targeted Q4 2026 (October 2026); clearance target Q2–Q3 2027 (June 2027 estimate).
Not currently FDA-cleared. No claims of regulatory clearance until after FDA review. No claims about medical-device status until post-clearance.
Intellectual property
Provisional patent filing targeted May 15, 2026 — three claim families covering distributed inference + safety architecture, emotional gravity, and audio-native crisis detection.
Interested in partnering on the pilot, advising clinically, or funding the work?
Let's build the evidence together
Three ways to engage, depending on where you sit.